
Newsroom
Recent Press Releases

National Jewish Health recognized by U.S. News & World Report as a Top Hospital in Pulmonology for the 30th Consecutive Year

National Jewish Health Appoints R. Stanton Dodge as Chair of Board of Directors

National Jewish Health Advanced Diagnostic Laboratories Receives Re-Accreditation from College of American Pathologists

National Jewish Health Welcomes Vivian Lee, MD, to Gastroenterology Team

New Expert Recommendations Aim to Improve Detection and Care of Lung Disease in People with Rheumatoid Arthritis

Los Angeles Black & White Ball Raises $430,000 for National Jewish Health

National Jewish Health Researchers Discover New Driver of Asthma-Related Inflammation

National Jewish Health Crowns Mercedes-Benz of Denver First Winner of Inaugural Mile High Games

Study Finds Tezepelumab Helps Patients with Severe Asthma Reduce Oral Steroid Use While Maintaining Asthma Control

New Study Finds No Significant Joint Damage in Astronauts After Short-Duration Spaceflight, Highlighting Promise of Ultrasound Monitoring

National Jewish Health Study Finds Significant Global Burden of Silicosis Among Mineral Miners

National Jewish Health Welcomes Maggie Britton, PhD, as Clinical Director of Health Initiatives

Media Trailblazer Pat Mitchell to Be Honored at ‘A Breath of Fresh Air Gala’ on Sept. 2

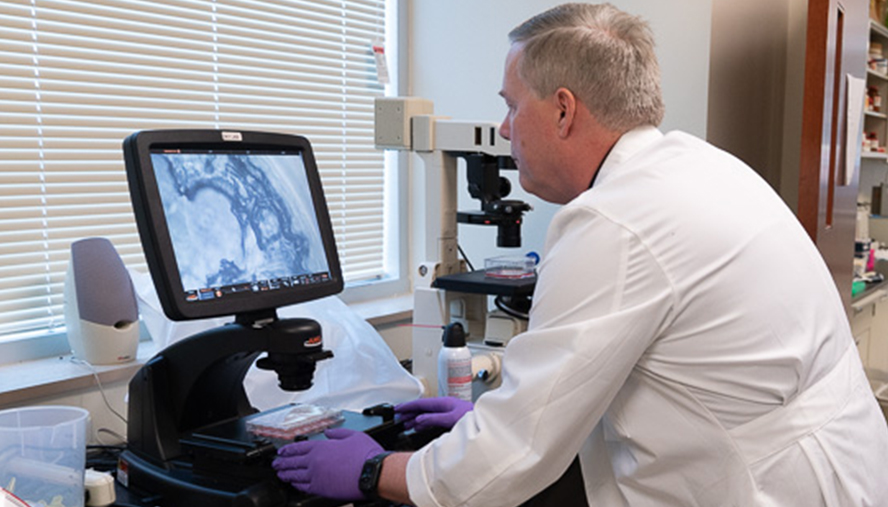
Lung Scans Can Reveal Important Differences in Sarcoidosis Severity According to New Study

National Jewish Health Welcomes Occupational and Environmental Medicine Specialist Erin Bammann, MD

Hoops and Hoopla Raises $130,000 to Benefit National Jewish Health Funds support Morgridge Academy, school for children with chronic illnesses

Advanced CT Scan Analysis May Help Identify Different Forms of Sarcoidosis

New Study Identifies Promising Pathway to Reverse Pulmonary Fibrosis

A Rockin’ 50s Beaux Arts Ball Raises More Than $2 Million to Benefit National Jewish Health

Intermountain Health Saint Joseph Hospital and National Jewish Health Pioneer AdvanceTherapy to Help COPD Patients Breathe Easier

Pulmonary and Critical Care Physician-Scientist Mary Elizabeth Richert Joins National Jewish Health

Dupilumab Restores Skin Barrier Function in Children with Moderate-to-Severe Atopic Dermatitis, Study Shows

Study Suggests Asthma LABA Medications Do Not Increase Severity of Food Allergy Reactions During Oral Food Challenges

Valentine’s Day Is the Perfect Time to Show Your Nose Some Love: Start Allergy Medications Now

A Cardiac Warning Sign: The One Big Tell of a Heart Attack vs. Heartburn

National Jewish Health Welcomes Radiologist Brian M. Smiley, MD
New Study Reveals How Burn Pit–Related Particulate Matter Triggers Harmful Lung Inflammation

Dr. Soonho Yoon, International Leader in Thoracic Imaging and Lung Disease Research, Joins National Jewish Health

Study Links Burn Pit Smoke Exposure to Increased Lung Particle Burden in Post-9/11 Veterans

Glen J. Weiss of Vornado Realty Trust Honored at the 57th Annual “A Winter’s Evening Dinner” Dance

Dr. Kristen Steslow Joins National Jewish Health Neurology & Behavioral Health Team

Community Asthma Program on Navajo Nation Increases Care-Seeking for Children with Asthma

Heartburn or Heart Attack: Symptoms Doctors Say You Can’t Ignore

Dr. Sohini Ghosh Joins the National Jewish Health Interventional Pulmonology Team

Rev the Runway Raises More Than $415,000 for National Jewish Health

Dr. Ivana Ilic Joins the National Jewish Health Rheumatology Team

National Jewish Health Expands Lung Cancer Screening Access and Hosts Saturday Screening Event

Dr. Joshua Nardin Joins the National Jewish Health Neurology Team

Study Identifies Viral Combinations That Heighten Risk of Severe Respiratory Illnesses in Infants

National Jewish Health Reaccredited as Pulmonary Hypertension Comprehensive Care Center

National Jewish Health Names Alex Hurst as Executive Director of Health Initiatives
National Jewish Health Earns WASOG Center of Excellence Award for Sarcoidosis

National Jewish Health Receives AHA 100-Year Milestone Award

Study Finds One-Year Change on CT Scans Linked to Future Outcomes in Fibrotic Lung Disease

Dr. Mark Lott Joins the National Jewish Health Behavioral Health Team

Dr. Vivianne Allsop Joins National Jewish Health Rheumatology Team

Dr. Joey Pryor Joins the National Jewish Health Pulmonology Team

Lt. Governor Dianne Primavera and National Jewish Health Host Long COVID Roundtable to Advance Care and Collaboration

Dr. Sarah Rhoads Joins the National Jewish Health Pulmonology Team

Common Cold May Protect Against COVID-19 According to National Jewish Health Researchers
Multimedia Story Assets



Upcoming Education Events
September
NTM & Bronchiectasis Conference for Healthcare Providers (Hybrid Event)
12:15PM
National Jewish Health - Molly Blank Conference Center
1400 Jackson Street, Denver, Colorado 80206NTM & Bronchiectasis: Patient & Family Course (Hybrid Event)
9:00AM
National Jewish Health - Molly Blank Conference Center
1400 Jackson Street, Denver, Colorado 80206October
22nd Annual Respiratory Disease Young Investigators’ Forum
8:00AM
Halcyon – A Hotel in Cherry Creek
245 Columbine St, Denver, Colorado 8020622nd Annual Respiratory Disease Young Investigators’ Forum
8:00AM
Halcyon – A Hotel in Cherry Creek
245 Columbine St, Denver, Colorado 80206February
49th Annual Pulmonary & Allergy Update
4:00PM
Keystone Conference Center
633 Tennis Club Road, Keystone, Colorado 80435March
63rd Annual Denver TB Course (Hybrid Event)
1:30PM
National Jewish Health - Molly Blank Conference Center
1400 Jackson Street, Denver, Colorado 80206